
A 50-year-old African man with well-controlled HIV infection presented with constitutional symptoms, progressive multiorgan failure, and raised inflammatory markers. He had a history of Kaposi sarcoma. An infective etiology was excluded.
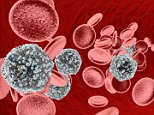
He had a rising white cell count and the blood film (panels A-B; May-Grünwald Giemsa stain; original magnification ×20 A and ×40 B) showed large cells with abundant, basophilic cytoplasm, irregular nuclei, and prominent nucleoli.
Immunophenotyping of the peripheral blood confirmed these cells to be λ-restricted plasma cells. Bone marrow biopsy demonstrated the same clonal plasma cells (panels C,E; May-Grünwald Giemsa stain, original magnification ×60 C; CD138 stain, original magnification ×20 E) and the presence of hemophagocytosis (panel D; May-Grünwald Giemsa stain; original magnification ×60). The main differential diagnoses were plasma cell myeloma or plasmablastic lymphoma, with the latter favored in the context of HIV infection.
A positron emission tomography computed tomography scan showed mild splenomegaly but no lymphadenopathy or effusions. Subsequent results revealed a human herpesvirus 8 (HHV8) viremia of 70 million copies/mL, Kaposi sarcoma in the skin, and occasional HHV8+ cell in the trephine (panel F; HHV8 stain; original magnification ×40).
Testing for Epstein-Barr virus was negative. The diagnosis was therefore revised to an HHV8-associated lymphoproliferative disorder, most likely multicentric Castleman disease. He was treated with 4 doses of rituximab and had a full clinical response. Castleman disease is known to involve the blood and bone marrow, but is only rarely seen without lymphadenopathy.


