
To avoid puncture of tendons, blood vessels, and nerves, the clinician performing the procedure should be familiar with the anatomy of the specific joint. The risk of such injuries can be minimized by using the extensor surface of the joint for needle insertion while keeping the joint in minimal flexion.
Background
Arthrocentesis (synovial fluid aspiration) of the knee can be performed either diagnostically (for identification of the etiology of acute arthritis) or therapeutically (for pain relief, drainage of effusion, or injection of medications).1, 2
Although this approach is not covered in this article, it seems that ultrasound-guided arthrocentesis and injection of the knee are superior to arthrocentesis and injection guided by anatomic landmarks and palpation, resulting in significantly less procedural pain, improved arthrocentesis success, greater synovial fluid yield, more complete joint decompression, and improved clinical outcomes.3
Indications
Indications for diagnostic knee arthrocentesis include the following:
-
Evaluation of monoarticular arthritis
- Evaluation of suspected septic arthritis
- Evaluation of joint effusion
- Identification of intra-articular fracture
- Identification of crystal arthropathy
Indications for therapeutic knee arthrocentesis include the following:
-
Relief of pain by aspirating effusion or hemarthrosis
- Injection of medications (eg, corticosteroids, antibiotics, or anesthetics)
- Drainage of septic effusion
Contraindications
There are no absolute contraindications for knee arthrocentesis. Relative contraindications include the following:
-
Cellulitis overlying the joint – If arthrocentesis is performed, the patient should be admitted for the administration of intravenous (IV) antibiotics, even if the synovial fluid is not suggestive of infectious arthritis
- Skin lesion or dermatitis overlying the joint
- Known bacteremia
- Adjacent osteomyelitis
- Uncontrolled coagulopathy
- Joint prosthesis – Preferably, a joint prosthesis is tapped by an orthopedist
Periprocedural Care
Equipment
The materials required for knee arthrocentesis include the following:
-
Sterile gloves and drapes
- Gauze pads (5), 4 × 4 in.
- Skin preparatory solution
- Lidocaine 1%
- Syringes, 5 mL, 20 mL, 30 mL, 60 mL
- Needles, 18 or 20 gauge and 25 or 27 gauge
- Patients who are morbidly obese might require a 21-gauge spinal needle for arthrocentesis
- Hemostat
- Specimen tubes
- Bandage
Patient Preparation
Anesthesia
Patients who are anxious, in severe pain, or unable to cooperate with the procedure (most commonly children) might require procedural sedation and/or analgesia.
Local anesthesia is always warranted. After skin preparation, draping, and identification of the needle insertion site, use a 25- or 27-gauge needle to inject 2-5 mL of local anesthetic (eg, lidocaine 1%) into the subcutaneous tissue (see the image below). (See Local Anesthetic Agents, Infiltrative Administration.) Deep injections that might enter the joint space are not recommended, because they may alter the synovial fluid analysis results.
Infiltration of local anesthetic via medial parapatellar approach (left knee).
Positioning
After obtaining informed consent, place the patient supine on a gurney. Place a rolled towel below the patient’s knee. A small but randomized study demonstrated that more joint fluid was aspirated from patients in the supine position than from patients in the sitting position.4
Technique
Approach Considerations
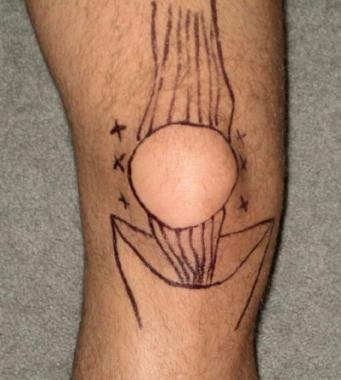
The clinician performing the procedure should be familiar with the anatomy of the specific joint and cognizant of the relevant landmarks in order to avoid puncture of tendons, blood vessels, and nerves (see the images below).
Anterior view of right knee.
Anatomic landmarks for knee arthrocentesis.
Aspiration of Synovial Fluid From Knee
Knee arthrocentesis may be done via a parapatellar approach (which is generally preferred),5, 6, a suprapatellar approach,2 or an infrapatellar approach. Once the insertion site is chosen, prepare the skin with sterile solution, allow drying, and then drape.
Using a sterile technique, attach the 18- or 20-gauge needle to the 20-mL syringe, and pull the plunger in order to break resistance. Because the knee may hold up to 70 mL of fluid, using a larger (60-mL) syringe is advisable in certain cases; accordingly, an extra syringe should be available for use if necessary.
Stretch the skin over the insertion site, and insert the needle briskly into the joint space while gently aspirating until synovial fluid enters the syringe (in an adult of average size, this usually occurs at 1-2 cm). Relaxation of the quadriceps muscle facilitates insertion of the needle. Placement of a towel under the popliteal region to flex the knee to 15-20° may facilitate entry by opening up the joint space.
For the parapatellar approach, identify the midpoint of either the medial or the lateral border of the patella. Insert an 18-gauge needle 3-4 mm below the midpoint of either the medial or the lateral border of the patella (see the image below). Direct the needle perpendicular to the long axis of the femur and toward the intercondylar notch of the femur.
Left-knee aspiration via medial parapatellar approach.
For the suprapatellar approach, identify the midpoint of either the superomedial or the superolateral border of the patella. Insert an 18-gauge needle through the midpoint of either set of superior borders. Direct the needle toward the intercondylar notch of the femur. With this approach, the needle enters the suprapatellar bursa. Remember that in 10% of the population, the suprapatellar bursa does not communicate with the knee joint.
For the infrapatellar approach, position the patient sitting upright with the knee bent at 90° over the edge of the bed. Identify either side of the inferior border of the patella and the patellar tendon. Insert an 18-gauge needle 5 mm below the inferior border of the patella and just lateral to the edge of the patellar tendon. Be careful not to go through the patellar tendon while inserting the needle.
If a bone is encountered during needle insertion, pull the needle back, verify the anatomic landmarks, and advance the needle in a corrected direction.
If fluid stops flowing into the syringe, attempt to “milk” the suprapatellar region by applying gentle pressure to the region.
If removal of more fluid is desired, a hemostat can be used to secure the needle in place while the syringe is replaced with a new one.
Once aspiration is complete, the needle is removed and a bandage applied (see the image below).
Application of bandage after left-knee aspiration.
Analysis of Synovial Fluid
The aspirated synovial fluid is then analyzed (see Table 1 below).7, 8
Table 1. Characteristics of Synovial Fluid on Analysis (Open Table in a new window)
| Appearance | WBCs, cells/µL | PMN cells | Glucose concentration, mg/dL | Protein concentration, g/dL | |
| Normal | Clear | <150 | <0.25 | Serum glucose | 1.3-1.8 |
| Noninflammatory | Clear | <3000 | <0.25 | Serum glucose | 2-3.5 |
| Inflammatory | Cloudy | >3000 | <0.75 | <25 | >4 |
| Purulent | Cloudy | >50,000 | >0.9 | <25 | >4 |
| Hemorrhagic | Bloody | >2000 | ~0.3 | Serum glucose | … |
| PMN = polymorphonuclear; WBC = white blood cell. | |||||
Synovial fluid characteristics associated with septic joint effusion are as follows:
-
Total white blood cell (WBC) count higher than 25,000/µL (sensitivity, 77%; specificity, 73%; positive likelihood ratio LR +, 29; negative likelihood ratio LR –, 0.71)
- Total WBC count higher than 50,000/µL (sensitivity, 62%; specificity, 92%; LR +, 7.7; LR –, 0.42) 9
- Total WBC count higher than 100,000/µL (sensitivity, 22%; specificity, 99%; LR +, 2.9; LR –, 0.32)
- PMN cell proportion 0.9 or higher (sensitivity, 73%; specificity, 79%; LR +, 3.4; LR –, 0.34)
- Synovial glucose or serum glucose concentration lower than 0.5 (sensitivity, 51%; specificity, 85%; LR +, 3.4; LR –, 0.58)
- Protein concentration higher than 3 g/dL (sensitivity, 48%; specificity, 46%; LR +, 0.9; LR – -, 1.1)
- Lactic dehydrogenase (LDH) concentration higher than 250 U/L (sensitivity, 100%; specificity, 51%; LR +, 1.9; LR –, 0.1)
Complications
Improper needle placement, a small amount of effusion, or mechanical obstruction of the needle against cartilage or thickened synovium can cause a dry tap.
Potential damage to cartilage can be avoided by understanding the joint anatomy and avoiding further advancement of the needle into the joint space once synovial effusion enters the syringe.
Most hemarthroses are small and self-limited and can be managed with observation alone. Hemarthrosis in coagulopathic patients requires correction of the coagulopathy in consultation with a hematologist.
With proper skin cleansing and the use of aseptic technique, the risk of introducing infection into a sterile joint can be reduced to less than 1:10,000.
When arthrocentesis is performed through infected skin for the diagnosis of a potentially septic joint, intravenous antibiotics should be administered immediately after the procedure, and the patient should be admitted for continuation of the antibiotics.
Medication
Medication Summary
The goals of pharmacotherapy are to reduce morbidity and prevent complications.
Local Anesthetics, Amides
Class Summary
Local anesthetics block the initiation and conduction of nerve impulses.
Lidocaine (Xylocaine)
Lidocaine is an amide local anesthetic used in 1-2% concentration. The 1% preparation contains 10 mg of lidocaine for each 1 mL of solution; the 2% preparation contains 20 mg of lidocaine for each 1 mL of solution. Lidocaine inhibits depolarization of type C sensory neurons by blocking sodium channels.
To improve local anesthetic injection, cool the skin with ethyl chloride before injection. Use a 25- or 27-gauge needle to inject 2-5 mL of local anesthetic (eg, lidocaine 1%) into the subcutaneous tissue. Make sure the solution is at body temperature. Infiltrate very slowly to minimize the pain. The time from administration to onset of action is 2-5 minutes, and the effect lasts for 1.5-2 hours.
Buffering the solution helps reduce the pain of local lidocaine injection. Sodium bicarbonate can be added to injectable lidocaine vials (1 part bicarbonate to 9 parts lidocaine) to produce buffered lidocaine. The shelf-life of buffered lidocaine is approximately 1 week at room temperature. All vials should be marked “buffered,” labeled with the time and date, and signed by the person who created the buffered mixture.
References
- Siva C, Velazquez C, Mody A, Brasington R. Diagnosing acute monoarthritis in adults: a practical approach for the family physician. Am Fam Physician. 2003 Jul 1. 68(1):83-90. Medline. Full Text.
- Zuber TJ. Knee joint aspiration and injection. Am Fam Physician. 2002 Oct 15. 66(8):1497-500, 1503-4, 1507. Medline. Full Text.
- Sibbitt WL Jr, Kettwich LG, Band PA, Chavez-Chiang NR, DeLea SL, Haseler LJ, et al. Does ultrasound guidance improve the outcomes of arthrocentesis and corticosteroid injection of the knee?. Scand J Rheumatol. 2012 Feb. 41(1):66-72. Medline.
- Zhang Q, Zhang T, Lv H, Xie L, Wu W, Wu J, et al. Comparison of two positions of knee arthrocentesis: how to obtain complete drainage. Am J Phys Med Rehabil. 2012 Jul. 91(7):611-5. Medline.
- Self WH, Wang EE, Vozenilek JA, del Castillo J, Pettineo C, Benedict L. Dynamic emergency medicine. Arthrocentesis. Acad Emerg Med. 2008 Mar. 15(3):298. Medline.
- Thomsen TW, Shen S, Shaffer RW, Setnik GS. Videos in clinical medicine. Arthrocentesis of the knee. N Engl J Med. 2006 May 11. 354(19):e19. Medline.
- Margaretten ME, Kohlwes J, Moore D, Bent S. Does this adult patient have septic arthritis?. JAMA. 2007 Apr 4. 297(13):1478-88. Medline.
- Li SF, Cassidy C, Chang C, Gharib S, Torres J. Diagnostic utility of laboratory tests in septic arthritis. Emerg Med J. 2007 Feb. 24(2):75-7. Medline.
- McGillicuddy DC, Shah KH, Friedberg RP, Nathanson LA, Edlow JA. How sensitive is the synovial fluid white blood cell count in diagnosing septic arthritis?. Am J Emerg Med. 2007 Sep. 25(7):749-52. Medline.



Hi, it’s Craig again!
I’m writing because I want to comment on the good work on the septic content on osvilt.com. Things are getting a bit stale though… and Google just updated their algorithm yet again, you know how that’ll impact your biggest free traffic source, if there isn’t an ongoing flow of new blogs! You see, most websites get majority of their organic traffic from their blogs, and I feel that you could use a little help, since you are not blogging constantly yet.
Blogging takes a lot of time and energy, and we have just the team from US/Canada to come up with awesome content you are looking for.
You can have a brand new blog to post on your website starting at $10 in as little as 5 business days!
I have learned result-oriented things by your blog. One other thing I would like to say is the fact that newer laptop or computer operating systems are likely to allow much more memory for use, but they as well demand more ram simply to work. If people’s computer can’t handle a lot more memory as well as the newest program requires that memory increase, it usually is the time to buy a new Personal computer. Thanks
Wow that was strange. I just wrote an very long comment but after I clicked submit my comment didn’t appear. Grrrr… well I’m not writing all that over again. Anyhow, just wanted to say fantastic blog!
Vielen Dank für den tollen Artikel.
Wow! Thank you! I permanently needed to write on my website something like that. Can I implement a portion of your post to my website?
Good day! Do you use Twitter? I’d like to follow you if that would be ok. I’m absolutely enjoying your blog and look forward to new updates.
Thanks for the sensible critique. Me & my neighbor were just preparing to do a little research about this. We got a grab a book from our area library but I think I learned more clear from this post. I’m very glad to see such fantastic information being shared freely out there.
After study a number of of the blog posts in your web site now, and I actually like your method of blogging. I bookmarked it to my bookmark website record and will be checking again soon. Pls take a look at my website as well and let me know what you think.