Treatment of atherosclerotic cardiosclerosis is reduced to pathogenetic therapy of individual syndromes – heart failure, hypercholesterolemia, arrhythmias, atrioventricular block, etc. With this purpose, diuretics, nitrates, peripheral vasodilators, statins, antiarrhythmic drugs are prescribed.
The constant intake of antiplatelet agents (acetylsalicylic acid) is obligatory.
Important factors in the complex treatment of atherosclerotic cardiosclerosis are diet therapy, adherence, and physical exercise restrictions. Balneotherapy is indicated for such patients – carbon dioxide, hydrosulphuric, radon, pine baths.
During the formation of an aneurysmal defect of the heart, surgical resection of the aneurysm is performed. For persistent disturbances in rhythm and conduction, implantation of an EKS or cardioverter defibrillator may be required; in some forms, radiofrequency ablation (RFA) contributes to the restoration of normal rhythm.
Cardiosclerosis (myocardiosclerosis) is a process of focal or diffuse replacement of myocardial muscle fibers with connective tissue. Taking into account the etiology, it is customary to distinguish between myocarditis (due to myocarditis, rheumatism), atherosclerotic, post-infarction and primary (with congenital collagenosis, fibroelastosis) cardiosclerosis. Atherosclerotic cardiosclerosis in cardiology is considered as a manifestation of coronary heart disease caused by the progression of coronary atherosclerosis. Atherosclerotic cardiosclerosis is detected predominantly in males of middle and old age.
Atherosclerotic cardiosclerosis is a diffuse development of connective scar tissue in the myocardium due to atherosclerotic lesions of the coronary arteries. Atherosclerotic cardiosclerosis is manifested by progressive ischemic heart disease: strokes, rhythm and conduction disturbances, heart failure. Diagnosis of atherosclerotic cardiosclerosis includes a set of instrumental and laboratory tests – ECG, echoCG, bicycle ergometry, pharmacological tests, the study of cholesterol and lipoproteins. Treatment of atherosclerotic cardiosclerosis is conservative; It is aimed at improving the coronary circulation, normalizing rhythm and conduction, reducing cholesterol, relieving pain syndrome.
Causes of Atherosclerotic Cardiosclerosis
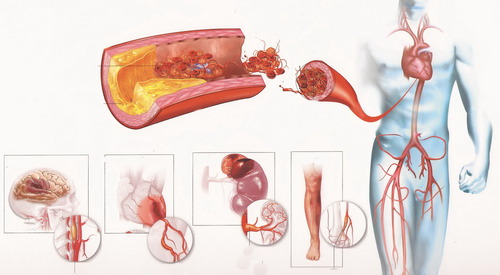
Atherosclerotic lesion of the coronary vessels is the basis of the pathology under consideration. The leading factor in the development of atherosclerosis is a violation of cholesterol metabolism, accompanied by excessive deposition of lipids in the inner lining of blood vessels.
The rate of formation of atherosclerosis of the coronary vessels is significantly influenced by concomitant arterial hypertension, a tendency to vasoconstriction, and excessive consumption of cholesterol-rich foods.
Atherosclerosis of the coronary vessels leads to a narrowing of the lumen of the coronary arteries, impaired blood supply to the myocardium, followed by the replacement of muscle fibers with scar connective tissue (atherosclerotic cardiosclerosis).
Pathogenesis of atherosclerotic cardiosclerosis
Stenosing atherosclerosis of the coronary arteries is accompanied by ischemia and metabolic disorders in the myocardium, and, as a result, by gradual and slowly developing dystrophy, atrophy and death of muscle fibers, in the place of which necrosis areas and microscopic ribs are formed. The death of receptors helps to reduce the sensitivity of myocardial tissues to oxygen, which leads to further progression of coronary artery disease.
Atherosclerotic cardiosclerosis is diffuse and prolonged. With the progression of atherosclerotic cardiosclerosis, compensatory hypertrophy develops, and then dilatation of the left ventricle, signs of heart failure increase.
Taking into account the pathogenetic mechanisms, ischemic, post-infarction and mixed variants of atherosclerotic cardiosclerosis are distinguished. Ischemic cardiosclerosis develops due to prolonged circulatory failure, progresses slowly, diffusely affecting the heart muscle. Postinfarction (postnecrotic) cardiosclerosis is formed at the site of the former site of necrosis. Mixed (transient) atherosclerotic cardiosclerosis combines both of the above mechanisms and is characterized by a slow diffuse development of fibrous tissue, against the background of which necrotic foci form periodically after repeated myocardial infarction.
Symptoms of atherosclerotic cardiosclerosis
Atherosclerotic cardiosclerosis manifests itself in three groups of symptoms indicating a violation of the contractile function of the heart, coronary insufficiency and disorders of rhythm and conduction. The clinical symptoms of atherosclerotic cardiosclerosis for a long time can be expressed slightly. Later, chest pains radiating to the left arm, to the left scapula, to the epigastric region occur. Repeated myocardial infarction may develop.
As the scar-sclerotic process progresses, increased fatigue appears, shortness of breath (first – with heavy physical exertion, then – with normal walking), often – attacks of cardiac asthma, pulmonary edema. With the development of heart failure, congestion in the lungs, peripheral edema, hepatomegaly, and in severe forms of atherosclerotic cardiosclerosis – pleurisy and ascites join.
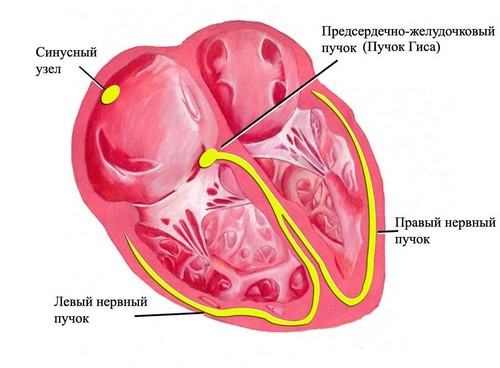
Cardiac rhythm and conduction disorders in atherosclerotic cardiosclerosis are characterized by a tendency to the occurrence of extrasystole, atrial fibrillation, intraventricular and atrioventricular blockades. Initially, these violations are paroxysmal in nature, then become more frequent, and later – permanent.
Atherosclerotic cardiosclerosis is often combined with atherosclerosis of the aorta, cerebral arteries, large peripheral arteries, which is manifested by appropriate symptoms (memory loss, dizziness, intermittent claudication, etc.).
Atherosclerotic cardiosclerosis carries a slowly progressive course. Despite possible periods of relative improvement, which can last for several years, repeated acute disorders of the coronary circulation lead to a deterioration of the condition.
Diagnosis of atherosclerotic cardiosclerosis
The diagnosis of atherosclerotic cardiosclerosis is based on anamnesis (IHD, atherosclerosis, arrhythmias, myocardial infarction, etc.) and subjective symptoms. Biochemical blood test revealed hypercholesterolemia, an increase in beta-lipoproteins.
On an ECG, signs of coronary insufficiency, post-infarction scars, rhythm disturbances and intracardiac conduction, moderate left ventricular hypertrophy are determined. The data of echocardiography in atherosclerotic cardiosclerosis are characterized by impaired myocardial contractility (hypokinesia, dyskinesia, akinesia of the corresponding segment). Veloergometry allows you to specify the degree of myocardial dysfunction and functional reserves of the heart.
The performance of pharmacological tests, daily ECG monitoring, polycardiography, rhythmocardiography, ventriculography, coronary angiography, MRI of the heart, and other studies can contribute to solving diagnostic problems in atherosclerotic cardiosclerosis. To clarify the presence of effusion, ultrasound of the pleural cavity, chest x-ray, and abdominal ultrasound are performed.
Prognosis and prevention of atherosclerotic cardiosclerosis
The prognosis of atherosclerotic cardiosclerosis depends on the extent of the lesion, the presence and type of arrhythmia and conduction, and the stage of circulatory failure.
The primary prevention of atherosclerotic cardiosclerosis is the prevention of atherosclerotic vascular changes (proper nutrition, sufficient physical activity, etc.).
Measures of secondary prevention include rational therapy of atherosclerosis, pain, arrhythmias and heart failure. Patients with atherosclerotic cardiosclerosis require systematic observation by a cardiologist, examination of the cardiovascular system.