Since the spontaneous closure of the aortic pulmonary defect is impossible, the only way to treat congenital heart disease is cardiac surgery. With a large defect of the aortic pulmonary septum, the operation is carried out in early terms – up to 1 year.
Aortic pulmonary window closure is performed by suturing or plastics of the defect using patches accessed through the lumen of the aorta or pulmonary artery, or on both sides. The operation is performed in terms of IR, hypothermia and pharmaco-cold cardioplegia.
In the event of a defect in the aortic pulmonary septum type I, the duct is ligated.
The impossibility of performing a radical operation with pulmonary hypertension dictates the need for a two-stage intervention: 1 – narrowing of the pulmonary trunk or pulmonary artery; 2 – removal of the narrowing cuff and radical surgery.
Intraoperative mortality is 3%; postoperative reaches 15-20%.
The defect of the aorto-pulmonary septum (aorto-pulmonary window, aortopulmonary septal defect, aorto-pulmonary fistula or fenestration) is due to the presence of a hole through which the aorta and the pulmonary artery communicate with each other. The defect of the aortic pulmonary septum is a rare abnormality, which in cardiology constitutes 0.2–0.3% of cases of all congenital heart defects.
Localization of the pathological message may be different: the defect in the aorto-pulmonary septum may be located anywhere between the adjacent sections of the ascending aorta and the pulmonary artery trunk. Defects of the aortic pulmonary septum differ in shape and size and can reach a diameter of 2 to 30 mm.
In almost half of the cases, the aortic pulmonary defect is combined with other congenital anomalies of the heart – an interventricular septal defect, an open arterial duct, Fallot’s tetrade, aortic coarctation, aortic subvalvular stenosis, pulmonary stenosis, etc.
Aortic pulmonary defect is a congenital cardiac anomaly, consisting in the presence of communication between the ascending aorta and the pulmonary artery adjacent to it. Defect of the aortic pulmonary septum manifests itself at an early age with shortness of breath, a delay in physical development, repeated pneumonia, the formation of a “heart hump”, cyanosis. Detection of aortic pulmonary defect is carried out on the basis of EchoCG, cardiac catheterization, aortography, ECG, PCG, X-ray, auscultation. With this defect, cardiac surgery is indicated – closure of the aortic pulmonary window by suturing or plastic repair of the defect.
Causes of aortic pulmonary defect
Arotropulmonary window is a consequence of a violation of embryogenesis, as a result of which a full-fledged aortic pulmonary septum is not formed. The separation of the embryonic arterial trunk into the aorta and pulmonary trunk occurs between 6-7 weeks of intrauterine development of the fetus. Violation of this process leads to a defect in the aortic pulmonary septum.
The causes of the development of aortic pulmonary defect are similar to those in the formation of other congenital heart defects.
Factors that disrupt the formation of the heart of the fetus in the early stages of fetal development may be infections of the pregnant woman (rubella, chicken pox, herpes, influenza, syphilis, etc.), alcohol intake and toxic drugs, somatic diseases of the mother (diabetes mellitus), pathological gestation (threat of spontaneous interruption, strong toxicoses), heredity, ionizing radiation, etc.
Features of hemodynamics with aortic pulmonary septal defect
The morphological criteria for aortic pulmonary defect are: pathological communication between the adjacent departments of the ascending aorta and the pulmonary trunk, the presence of isolated fibrous rings of the aortic and pulmonary valves and the formed excretory sections of both ventricles.
The last symptom distinguishes this defect from the common arterial trunk. The defect itself in the aortic pulmonary septum is an oval or circular opening with an intrapericardial location between the left wall of the ascending aorta and the right wall of the pulmonary trunk.
The severity of hemodynamic disturbances in aortic pulmonary septal defect depends on the size of the message, its location, the ratio of general and peripheral vascular resistance.
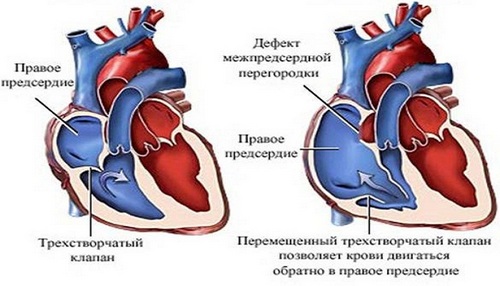
In case of aortic pulmonary defect, blood under high pressure enters from the ascending aorta into the pulmonary artery. A pronounced arteriovenous (left-right) discharge early leads to the development of pulmonary hypertension, which is present in most patients with aortic pulmonary septal defect. When the resistance in the small and large circulation is equalized, there is a cross, and then a venoarterial (right-left) discharge of blood, which is accompanied by the development of cyanosis.
Classification of aortic pulmonary defect
Taking into account the localization criteria, the shape of the hole and its relationship to the pulmonary arteries, the following anatomical types of aortic pulmonary defect are distinguished (V.I. Burakovsky et al., N. Bakulev NTSSSKH):
- Type I – the defect has the shape of a duct with well-defined poles; located in the middle of the aortic pulmonary septum away from the sinuses of Valsalva. The left and right pulmonary arteries depart distal to the aortic pulmonary defect.
- Type II – the defect has the shape of a window; located in the proximal (lower) part of the aorto-pulmonary septum above the sinuses of Valsalva. Aortic pulmonary septum partially formed in its distal part; branches of the pulmonary artery depart normally, distal to the defect.
- Type III – the defect has the shape of a window; It is located in the distal (upper) part of the aortic pulmonary septum at a distance from the sinuses of Valsalva. Aortic pulmonary septum partially formed in its proximal part. The branches of the pulmonary artery depart in the area of the top of the defect.
- Type IV – the defect has the shape of a window; located in the distal (upper) part of the aorto-pulmonary septum, at the level of discharge of the right branch of the pulmonary trunk. With this type of aortic pulmonary defect, the aorta communicates with both the right pulmonary artery and the common pulmonary trunk.
- Type V – the complete absence of the aortic pulmonary septum, but the valves of the aorta and the pulmonary artery are formed and separated. The pulmonary arteries depart from the common main vessel, originating from the base of the heart.
Symptoms of aortic pulmonary septal defect
In children of the first months of life, an early symptom of aortic pulmonary septal defect is dyspnea of the tachypnea type. Lagging in physical development, rapid fatigability, frequent acute respiratory viral infections, repeated pneumonia are characteristic.
At the stage of predominant arteriovenous discharge, the skin is of a physiological color or somewhat pale. A small cyanosis can appear with screaming, crying, cardiac and respiratory failure.
With the development of cross and venoarterial discharge of blood, cyanosis of the skin and visible mucous membranes becomes pronounced and permanent. In 70% of patients with aortic pulmonary defect, a chest heart-like hump-type deformity is detected, the formation of which is associated with an increase in the right ventricle operating in hyperfunction mode.
With a defect in the aortic pulmonary septum of small diameter and in children a satisfactory condition is maintained for a long time. With large defects, pulmonary hypertension develops early. The life expectancy of patients with aortic pulmonary septal defect depends on the size of the hole and ranges from several months to 30-40 years (on average, 14 years).
Diagnosis of aortic pulmonary defect
On examination of patients with aortic pulmonary septal defect, there is a lag in mass and height, a protrusion of the chest in the form of a heart hump. Percussion revealed the expansion of the boundaries of cardiac dullness in both directions; during auscultation, systolic murmur with a diastolic component, a change in heart tones are heard; palpation is determined systolic tremor in the II-III intercostal space.
With the help of phonocardiography, the auscultatory picture is fixed, as described above. Electrocardiography reveals signs of overloading of the right heart, hypertrophy of both ventricles, deviation of EOS to the right. The X-ray picture of the defect in the aorto-pulmonary septum is typical: an increase in the shadow of the heart, an extension of the aorta and pulmonary artery, an increase in the pulmonary pattern in the early period of the disease and its impoverishment in the development of pulmonary hypertension. With the help of echocardiography, a defect in the aorto-pulmonary septum is detected, the window is positioned, its size, and concomitant heart defects are excluded.
By sensing the cavities of the heart is determined by the severity of pulmonary hypertension, the magnitude of the discharge of blood, examines the degree of blood saturation with oxygen in the pulmonary artery. The diagnostic sign of aortic pulmonary defect is the possibility of a catheter from the pulmonary artery through the opening in the initial sections of the ascending aorta. When performing aortography, the penetration of a contrast agent from the ascending aorta into the pulmonary artery trunk is seen. Differential diagnosis of aortic pulmonary septal defect is carried out with VSD, common arterial trunk, open arterial duct.
Prediction of aortic pulmonary septal defect
The large size of the aortic pulmonary defect causes a malignant course of the disease: 25-30% of patients die within the first six months of life.
The causes of death of patients with aortic pulmonary defect are usually heart failure, rupture of aneurysm of the pulmonary artery into the pericardial cavity, cardiac tamponade (hemopericardium), thromboembolism, and bacterial endocarditis.
In the surviving patients, the absence of surgical treatment leads to the development of irreversible changes in the lungs, making surgical treatment impossible at a later date. In the literature, there are isolated indications for patients with aortic pulmonary defect, who have lived to 35−40 years.