In the preoperative period, cardiac glycosides, anticoagulants (subcutaneous heparin), antihypertensive drugs, oxygen therapy, oxygen therapy and barium are prescribed to patients with heart aneurysms.
Surgical treatment of acute and subacute cardiac aneurysm is indicated in connection with the rapid progression of heart failure and the threat of rupture of the aneurysmal sac. In chronic heart aneurysms, surgery is performed to prevent the risk of thromboembolic complications and to revascularize the myocardium.
As a palliative intervention resorted to strengthening the wall of the aneurysm with the help of polymeric materials. Radical operations include resection of a ventricular aneurysm or atrium (if necessary, followed by reconstruction of the myocardial wall with a patch), Culey septoplasty (with aneurysm of the interventricular septum).
When a false or post-traumatic aneurysm of the heart is suturing the heart wall. If necessary, additional revascularization intervention simultaneously perform resection of the aneurysm in combination with CABG. After resection and plastics of the heart aneurysm, the development of low ejection syndrome, repeated myocardial infarction, arrhythmias (paroxysmal tachycardia, atrial fibrillation), suture failure and bleeding, respiratory failure, renal failure, cerebral thromboembolism of the brain are possible.
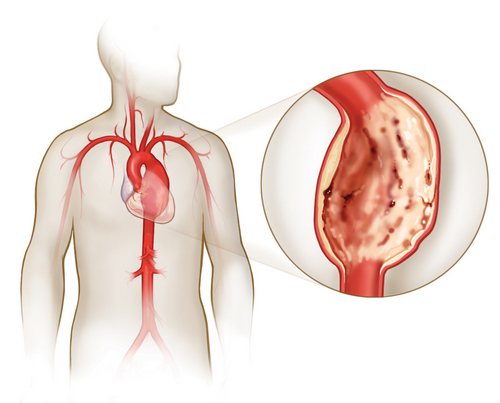
Aneurysm of the heart – a limited protrusion of the thinned wall of the myocardium, accompanied by a sharp decrease or complete disappearance of the contractile ability of the pathologically changed part of the myocardium. In cardiology, cardiac aneurysm is detected in 10-35% of patients who have had a myocardial infarction; 68% of acute or chronic heart aneurysms are diagnosed in men aged 40 to 70 years. Most often, aneurysm of the heart is formed in the wall of the left ventricle, less often in the area of the interventricular septum or right ventricle. The size of the aneurysm of the heart varies from 1 to 18-20 cm in diameter. Disturbance of myocardial contractility in the area of cardiac aneurysm includes akinesia (absence of contractile activity) and dyskinesia (protrusion of the aneurysm wall into systole and its depression into diastole).
Aneurysm of the heart – thinning and bulging of the myocardium of the heart chamber. Aneurysm of the heart can manifest as shortness of breath, palpitations, orthopnea, cardiac asthma, severe cardiac arrhythmias, thromboembolic complications. The main diagnostic methods for cardiac aneurysm are ECG, echoCG, chest x-ray, ventriculography, CT, MRI. Treatment of a heart aneurysm involves the excision of an aneurysmal sac with a closure of a defect in the heart muscle.
Causes of Aneurysm of the Heart
In 95-97% of cases, extensive transmural myocardial infarction, mainly of the left ventricle, is the cause of the heart aneurysm. The vast majority of aneurysms are localized in the area of the anterior-lateral wall and the apex of the left ventricle of the heart; about 1% – in the area of the right atrium and ventricle, interventricular septum and posterior wall of the left ventricle.
Massive myocardial infarction causes destruction of the structures of the muscular wall of the heart. Under the influence of the force of intracardiac pressure, the necrotic wall of the heart is stretched and thinned. A significant role in the formation of the aneurysm belongs to factors contributing to an increase in the load on the heart and intraventricular pressure – early rising, hypertension, tachycardia, repeated heart attacks, progressive heart failure.
The development of chronic heart aneurysm is etiologically and pathogenetically associated with post-infarction cardiosclerosis. In this case, under the action of blood pressure, a protrusion of the heart wall occurs in the region of the connective tissue scar.
Congenital, traumatic and infectious aneurysms are much less common than postinfarction heart aneurysms. Traumatic aneurysms are caused by closed or open injuries of the heart. Postoperative aneurysms that often occur after surgery to correct congenital heart defects (Fallot’s tetrad, pulmonary stenosis, etc.) can be attributed to this group.
Cardiac aneurysms caused by infectious processes (syphilis, bacterial endocarditis, tuberculosis, rheumatism) are very rare.
Classification of heart aneurysms
By the time of occurrence distinguish acute, subacute and chronic heart aneurysm. Acute heart aneurysm is formed in the period from 1 to 2 weeks from myocardial infarction, subacute – within 3-8 weeks, chronic – over 8 weeks.
Acute aneurysm
In the acute period, the aneurysm wall is represented by a necrotized myocardial site, which, under the action of intraventricular pressure, swells outwards or into the ventricular cavity (if the aneurysm is localized in the interventricular septum).
Sharp aneurysm
The wall of the subacute cardiac aneurysm is formed by a thickened endocardium with a cluster of fibroblasts and histiocytes, newly formed reticular, collagen and elastic fibers; in place of the destroyed myocardial fibers, connecting elements of varying degree of maturity are found.
Chronic aneurysm
Chronic cardiac aneurysm is a fibrous sac, microscopically consisting of three layers: endocardial, intramural and epicardial. In the endocardium of the wall of the chronic heart aneurysm there are growths of fibrous and hyalinized tissue. The wall of chronic aneurysm of the heart is thinned, sometimes its thickness does not exceed 2 mm. In the cavity of the chronic aneurysm of the heart, a near-wall thrombus is often found of various sizes, which can only lining the inner surface of the aneurysmal sac or occupy almost all of its volume. Loose parietal thrombi are easily fragmented and are a potential source of risk for thromboembolic complications.
There are three types of heart aneurysm: muscle, fibrous and fibromuscular. Typically, a heart aneurysm is single, although 2-3 aneurysms can be detected at a time. Aneurysms of the heart can be true (represented by three layers), false (formed as a result of rupture of the myocardial wall and limited to pericardial adhesions) and functional (formed by a section of viable myocardium with low contractility, swelling into ventricular systole).
Given the depth and extent of damage, a true heart aneurysm can be flat (diffuse), sacciform, mushroom-shaped, and in the form of an “aneurysm in aneurysm”. The diffuse aneurysm contour of the external protrusion is flat, gently sloping, and on the side of the heart cavity is determined by a deepening in the shape of a bowl. The saccular aneurysm of the heart has a rounded convex wall and a broad base.
Mushroom aneurysm is characterized by the presence of a large protrusion with a relatively narrow neck. The term “aneurysm in aneurysm” refers to a defect consisting of several protrusions that are enclosed one into another: such heart aneurysms have sharply thinned walls and are most prone to rupture. During the examination, diffuse aneurysms of the heart are more often detected, less often – sacciform and more rarely fungoid and “aneurysms in the aneurysm”.
Symptoms of aneurysm of the heart
Clinical manifestations of acute cardiac aneurysm are characterized by weakness, shortness of breath with episodes of cardiac asthma and pulmonary edema, prolonged fever, increased sweating, tachycardia, and heart rhythm disturbances (bradycardia and tachycardia, extrasystole, atrial fibrillation and ventricles, blockades). In a subacute heart aneurysm, the symptoms of circulatory failure progress rapidly.
The clinic of chronic aneurysm of the heart corresponds to pronounced signs of heart failure: shortness of breath, syncopal states, angina, rest and tension, feeling of interruptions in the work of the heart; in the late stage – neck vein swelling, edema, hydrothorax, hepatomegaly, ascites. In chronic aneurysm of the heart, fibrous pericarditis can develop, causing the development of adhesions in the chest cavity.
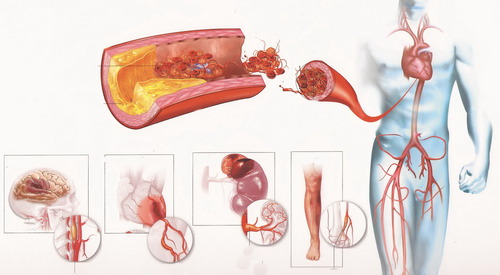
Thromboembolic syndrome in chronic heart aneurysm is represented by acute occlusion of the vessels of the extremities (usually the iliac and femoral-popliteal segments), the brachiocephalic trunk, the arteries of the brain, kidneys, lungs, intestines. Gangrene of the limb, stroke, renal infarction, pulmonary embolism, occlusion of the mesenteric vessels, repeated myocardial infarction can be potentially dangerous complications of chronic heart aneurysm.
Chronic heart aneurysm rupture is relatively rare. A rupture of an acute aneurysm of the heart usually occurs 2–9 days after myocardial infarction and is fatal. Clinically, the rupture of the heart aneurysm is manifested by a sudden onset: severe pallor, which is quickly replaced by cyanotic skin, cold sweat, overflow of neck veins with blood (evidence of cardiac tamponade), loss of consciousness, cooling of the extremities. Breathing becomes noisy, hoarse, shallow, sparse. Usually death comes instantly.
Diagnosis of heart aneurysm
Pathognomonic sign of a cardiac aneurysm is a pathological precordial pulsation, which is detected on the anterior wall of the chest and intensifies with each heartbeat.
Signs of transmural myocardial infarction are recorded on an ECG during cardiac aneurysm, which, however, do not change in stages, but retain a “frozen” character for a long time. EchoCG allows you to visualize the cavity of the aneurysm, measure its size, assess the configuration and diagnose ventricular cavity thrombosis. With the help of stress echoCG and PET of the heart, myocardial viability is detected in the area of chronic heart aneurysm.
Radiography of the chest reveals cardiomegaly, stagnation in the pulmonary circulation. Radiopaque ventriculography, MRI and MSCT of the heart are highly specific methods of topical diagnosis of aneurysm, determining its size, detecting thrombosis of its cavity.
According to the testimony of patients with cardiac aneurysm, heart cavities are probed, coronary angiography, EFI. Aneurysm of the heart must be differentiated from coelomic cysts of the pericardium, mitral heart disease, mediastinal tumors.
Prognosis and prevention of cardiac aneurysm
Without surgical treatment, a cardiac aneurysm is unfavorable: most patients with post-infarction aneurysms die within 2–3 years after the onset of the disease. Uncomplicated flat chronic aneurysms of the heart are relatively benign; the worst prognosis is saccular and fungoid aneurysms, often complicated by intracardiac thrombosis. Adherence of heart failure is an unfavorable prognostic sign.
Prevention of cardiac aneurysm and its complications consists in timely diagnosis of myocardial infarction, adequate treatment and rehabilitation of patients, gradual expansion of the motor regimen, control of rhythm disturbances and thrombus formation.