
Aspergillosis – a fungal infection caused by different types of moulds of the genus Aspergillus, and accompanied with chronic toxic-allergic manifestations.
When aspergillosis mainly affects bronchopulmonary system and paranasal sinuses; rarely skin, visual system, Central nervous system etc. in patients with low immune reactivity may develop disseminated aspergillosis.
A leading role in the diagnosis of aspergillosis play laboratory methods: microscopy, bacterial culture test, serological test, PCR. The possibility of setting inhalation and skin Allergy tests. Aspergillosis treatment is antifungal drugs.
Aspergillosis
Aspergillosis is a fungal disease, the causative agent of which are fungi Aspergillus. Aspergillus can cause a variety of superficial and deep mycoses of internal organs, skin and mucous membranes, therefore, the aspergillosis is studied in the framework of a variety of clinical disciplines: Mycology, pulmonology, otolaryngology, dermatology, ophthalmology, etc.
Over the past two decades, the rate of infection with aspergillosis in the population increased by 20% due to the increase in the number of patients with congenital and acquired immunodeficiency, drug use and HIV infection, irrational use of antibiotics, use of immunosuppressive drugs in Oncology and transplantation. This again confirms the increasing relevance of aspergillosis.
Causes of aspergillosis
Causative agents of aspergillosis in humans, there may be the following types of moulds of the genus Aspergillus: A. flavus, A. Niger, A. Fumigatus, A. nidulans. A. terreus, A. clavature. Aspergillus species are aerobic and heterotrophs; able to grow at temperatures up to 50°C continuously maintained during the drying and freezing. In the environment Aspergillus is ubiquitous in soil, air, water. Favorable conditions for growth and reproduction of Aspergillus are ventilation and shower systems, air conditioners and humidifiers, old things and books, damp walls and ceilings, long-stored food products, agricultural and room plants, etc.
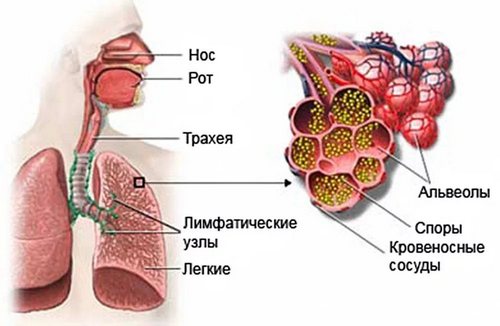
Infection, aspergillosis most often occurs by inhalation inhalation of dust particles containing fungal mycelium. The greatest risk of disease exposed to agricultural workers, workers in cotton-spinning and weaving companies, millers and breeders of pigeons, as pigeons, most birds, sick with aspergillosis. The emergence of fungal infection contributes to the infection when performing invasive procedures: bronchoscopy, puncture of paranasal sinuses, endoscopic biopsy, etc. are Not excluded contact transmission of aspergillosis infection through the damaged skin and mucous membranes. It is also possible alimentary infection with consumption of Aspergillus-contaminated food (e.g. chicken meat).

In addition to exogenous infection with Aspergillus, are known cases of autoparity (when activated fungi that live on the skin, mucous membrane of the throat and respiratory tract) and transplatzentarnogo infection. Risk factors in the incidence of aspergillosis include immunodeficiency of any origin, chronic diseases of the respiratory system (COPD, tuberculosis, bronchiectasis, bronchial asthma, etc.), diabetes mellitus, goiter, burn trauma; antibiotics, corticosteroids and cytotoxic drugs, radiotherapy. There are cases of development of fungal infections of mixed etiology, caused by different types of fungi – Aspergillus, Candida, actinomycetes.
Classification of aspergillosis
Thus, depending on the distribution of fungal infection distinguish endogenous (autoinfection), exogenous (airborne and alimentary way of transmission) and aspergillosis transplacental (vertical, by intrusion).
Localization of pathologic process there are distinguished the following forms of aspergillosis: a respiratory (including pulmonary aspergillosis), respiratory tract, skin, eye, bone, septic (generalized) and so On the primary lesion of the respiratory tract and lungs account for about 90% of all cases of aspergillosis; paranasal sinuses – 5%. Involvement of other organs is diagnosed less than 5% of patients; dissemination of aspergillosis develops in about 30% of cases, mainly in immunocompromised individuals with burdened premorbid background.
Symptoms of aspergillosis
The most studied to date form of disease is pulmonary aspergillosis. The initial stage bronchopulmonary aspergillosis masquerading as a clinic of tracheobronchitis or bronchitis. Patients with a cough with phlegm grayish color, hemoptysis, weakness, weight loss. With the spread of the lungs developing pulmonary form of the mycosis – aspergillosis pneumonia. In the acute phase, marked fever wrong type, chills, cough with abundant Muco-purulent sputum, shortness of breath, chest pain. When breathing through the mouth can be felt the smell of mold. With the help of microscopic examination of sputum found a colony of mycelium and spores of Aspergillus.
Patients with concomitant diseases of the respiratory system (pulmonary fibrosis, emphysema, cyst, lung abscess, sarcoidosis, tuberculosis, hypoplasia, histoplasmosis) often formed aspergilloma lung – encapsulated lesion containing mushroom hyphae, fibrin, mucus and cellular elements. The death of patients with aspergilloma may result from pulmonary hemorrhage or asphyxia.
Aspergillosis respiratory tract may occur in the form of external or otitis media, rhinitis, sinusitis, tonsillitis, pharyngitis. With Aspergillus otitis media in the beginning there is redness, flaking and itching of the skin of the external auditory canal. Over time the ear canal is filled with loose greyish mass containing filaments and spores. The possible spread of aspergillosis on the eardrum, causing a sharp stinging pain in the ear. Described lesions of the maxillary and sphenoid sinuses, the ethmoid bone, the transition of fungal invasion into the orbit. Ocular aspergillosis may take the form of conjunctivitis, blepharitis ulcerative, nodular keratitis, dacryocystitis, leveragability, panophthalmitis. Frequent complications in the form of deep ulcers of the cornea, uveitis, glaucoma, loss of vision.
Aspergillosis of the skin characterized by the appearance of erythema, infiltration, scales brownish, moderate itching. In the case of onychomycosis occurs deformation of the nail plate, color change to dark yellow or brownish-green, the crumbling of the nails. Aspergillosis of the gastrointestinal tract occurs under the form of erosive gastritis or enterocolitis: it is typical for a mildew smell from the mouth, nausea, vomiting, diarrhea.
Generalized form of aspergillosis develops in hematogenous dissemination of Aspergillus from the primary tumor in various organs and tissues. In this form of the disease occur aspergillosis endocarditis, meningitis, encephalitis; abscess of the brain, kidney, liver, myocardium; defeat of bones, gastrointestinal tract, ENT-organs; Aspergillus sepsis. Mortality from septic forms of aspergillosis is very high.
Diagnosis of aspergillosis
Depending on the shape of mycosis patients are referred for consultation to the specialist of the corresponding profile: pulmonologist, otolaryngologist, ophthalmologist, mycologist. In the process of diagnosis of aspergillosis much attention is paid to history, incl. professional, the presence of chronic lung disease and immunodeficiency. In cases of suspected bronchopulmonary form of aspergillosis conducted x-rays and lung CT scan, bronchoscopy with a sputum collection, bronchoalveolar lavage.
The basis for the diagnosis of aspergillosis is a set of laboratory research, material for which can serve as sputum, washings from the bronchial tubes, swabs with smooth skin and nails, discharge from sinuses, and external auditory meatus, prints from the surface of the cornea, feces, etc. Aspergillus can be detected by microscopy, cultural studies, PCR, serological tests (IFA, RSK, RIA). It is possible to conduct skin Allergy tests with antigens of Aspergillus.
Differential diagnosis of pulmonary aspergillosis is with inflammatory diseases of respiratory tract viral or bacterial etiology, sarcoidosis, candidiasis, pulmonary tuberculosis, cystic fibrosis, lung tumors etc. Aspergillosis of the skin and nails has similarities with athlete’s foot, rubromycosis, syphilis, tuberculosis, actinomycosis.
Treatment of aspergillosis
Depending on the severity of the patient and forms of aspergillosis treatment can be performed on an outpatient basis or in the hospital the corresponding profile. Therapy is antifungal drugs: amphotericin b, voriconazole, Itraconazole, flucytosine, caspofungin. Antifungal drugs can be given orally, intravenously, by inhalation. In the aspergillosis of the skin, nails and mucous membranes is local treatment of antifungals, antiseptics, enzymes. Antifungal therapy lasts 4 to 8 weeks, sometimes up to 3 months or longer.
In the aspergilloma of the lungs shown surgical tactics – the economical lung resection or lobectomy. In the treatment of any form of aspergillosis is necessary to conduct stimulating and immunocorrective therapy.
Forecast and prevention of aspergillosis
The most favorable course observed in the aspergillosis of the skin and mucous membranes. Mortality from pulmonary forms of mycosis is 20-35%, and in individuals with immunodeficiency – up to 50%. Septic form of aspergillosis has a poor prognosis. The measures to prevent infection with aspergillosis include measures to improve sanitary-hygienic conditions: dust control in manufacturing, the wearing by employees of the mills, granaries, storages, weaving enterprises personal protective equipment (respirators), improving the ventilation of workshops and warehouses, regular mycological examination of persons from risk groups.



But wanna remark on few general things, The website pattern is perfect, the content is very wonderful : D.
Hello!
Love the septic content on your site! You know, most businesses get traffic from their blogs, and we feel that you could use a little help, since you are not blogging daily yet.
Writing takes a lot of time, and we have just the team to come up with great content you need.
You can have your new article to post on your website starting at $10 in as little as 5 business days!
My programmer is trying to persuade me to move to .net from PHP.I have always disliked the idea because of the expenses.But he’s tryiong none the less. I’ve been using WordPress on a number of websites for about a year and am nervous about switching to another platform.I have heard great things about. Is there a way I can transfer all my wordpress content into it?Any kind of help would be greatly appreciated!
I am in fact grateful to the holder of this site who has shared this enormous article at here.
great issues altogether, you simply gained a new reader. What may you recommend in regards to your submit that you made some days ago? Any certain?
This is pretty interesting. Is it ok to volunteer a follow-up question?
With the help of microscopic examination of sputum found a colony of mycelium and spores of Aspergillus.
Actual working Clash of Clans Hack is tough to find among so many faux things.You have 30 seconds to assess the enemy base if it is worthattacking. The accumbent time arbor is actually scaled evenly.
Usually I don’t read article on blogs, but I wish to say that this write-up very forced me to try and do it! Your writing style has been amazed me. Thanks, quite nice post.
It?s hard to find knowledgeable people on this topic, but you sound like you know what you?re talking about! Thanks
After study a few of the blog posts on your website now, and I truly like your way of blogging. I bookmarked it to my bookmark website list and will be checking back soon. Pls check out my web site as well and let me know what you think.
With respect-thank you-Can you add to this?
An outstanding share! I’ve just forwarded this onto a colleague who had been doing a little homework
on this. And he actually ordered me breakfast
simply because I discovered it for him… lol.
So allow me to reword this…. Thanks for the
meal!! But yeah, thanx for spending some time
to discuss this matter here on your web site.